
Haemorrhoids are swollen blood vessels in and around the anus and lower rectum. In women they are common and very treatable, and they are often linked to pregnancy, childbirth, constipation and straining. Most cases settle with simple measures such as more fibre and fluids and warm baths, but persistent bleeding, a painful lump or symptoms that do not improve should be assessed by a doctor.
Key takeaways
- Haemorrhoids are very common — around half of adults experience them by about age 50.
- There are three main types: internal, external and thrombosed.
- Pregnancy and the period after childbirth are the most common female-specific triggers.
- Self-care helps most people; clinic procedures or surgery are reserved for cases that do not respond.
- Rectal bleeding should always be checked, especially from age 45 or with a family history of bowel cancer.
What Are Haemorrhoids?
Haemorrhoids, also called piles, are cushions of blood vessels that sit in and around the anal canal. Everyone has these cushions; the term “haemorrhoids” is used when they become swollen, irritated, or enlarged. They are one of the more common reasons people seek help for bowel-related symptoms, and they affect women and men alike.
Internal, External & Thrombosed
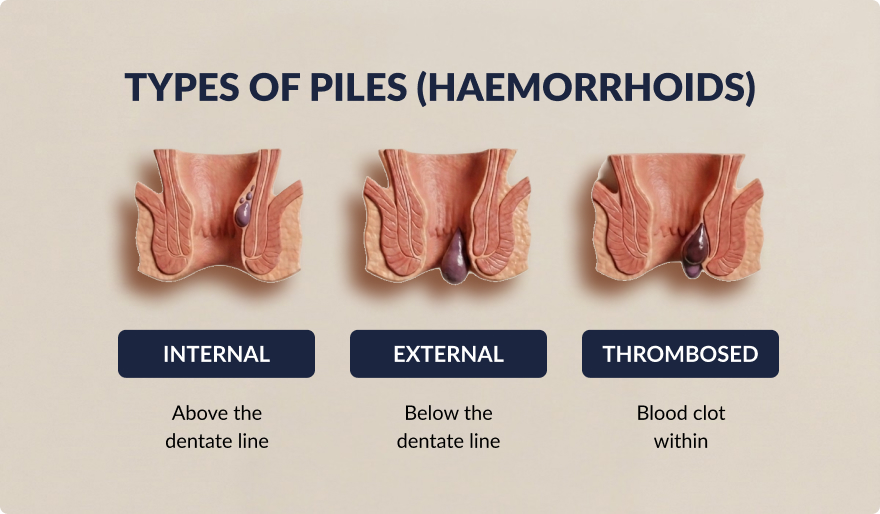
Haemorrhoids are grouped by where they form and what is happening to them:
- Internal haemorrhoids develop inside the rectum, above a landmark called the dentate line. Because this area has few pain nerves, they are often painless and may only show up as bright red bleeding. Larger internal haemorrhoids can bulge out (prolapse) during a bowel movement.
- External haemorrhoids form under the skin around the anal opening, below the dentate line. This skin is sensitive, so they can itch, ache or become sore.
- Thrombosed haemorrhoids occur when a blood clot forms inside an external haemorrhoid. This can come on suddenly and cause a firm, tender, bluish-purple lump.
Internal haemorrhoids are sometimes described in grades, from grade 1 (no prolapse) to grade 4 (prolapsed and cannot be pushed back). The type and grade help guide which treatment is most suitable.
Types of Haemorrhoids
What Do Haemorrhoids Look Like in Women?
Haemorrhoids look the same in women as in men — the difference is in what triggers them, not in their appearance.
- Internal haemorrhoids are usually out of sight inside the rectum, so you may not see anything at all. The first sign is often bright red blood on the toilet paper or in the bowl. If one prolapses, you may feel a small soft bulge at the anus that can sometimes be gently pushed back.
- External haemorrhoids can look or feel like one or more soft swellings, skin folds or lumps just around the anal opening.
- A thrombosed haemorrhoid typically appears as a single firm, swollen lump with a darker, bluish-purple tinge, and it is usually tender to touch.
Because other conditions — such as anal fissures, skin tags or, rarely, more serious causes — can produce similar symptoms, a doctor’s examination is the reliable way to confirm what you are seeing.
Symptoms in Women
Symptoms depend on the type of haemorrhoid and how irritated it is. Many women have only mild, occasional symptoms; others find them persistent and uncomfortable.
Internal vs External Symptoms
| Internal haemorrhoids | External haemorrhoids |
| Often painless | Can be itchy, sore or painful |
| Bright red bleeding during or after a bowel movement | A noticeable lump or swelling at the anus |
| A feeling of fullness or incomplete emptying | Discomfort when sitting |
| A soft bulge that may prolapse and return | Sudden severe pain if a clot forms (thrombosis) |
Bleeding, Prolapse & Pain
The most common symptoms women notice are:
- Itching and irritation around the anus, which can be persistent and hard to settle.
- Bleeding — usually bright red and small in amount, seen on the paper or in the bowl. Any rectal bleeding is worth having checked rather than assuming it is “just piles”.
- Pain or discomfort, particularly with external or thrombosed haemorrhoids, and sometimes when sitting for long periods.
- A lump or prolapse at the anus, soft with external haemorrhoids and firmer if a clot has formed.
- Discomfort during intercourse, which some women experience when an external haemorrhoid is present near the anal opening.
The symptoms themselves are broadly the same for women and men; what differs most is that pregnancy and childbirth give women extra reasons to develop them.
Common Causes in Women
Haemorrhoids develop when the blood vessel cushions around the anus come under repeated or increased pressure. Several everyday factors raise that pressure.
Pregnancy & After Birth
Pregnancy is the most common female-specific cause. As the uterus grows it presses on the pelvic blood vessels, while pregnancy hormones relax the vessel walls and slow the bowel, making constipation more likely. Straining during delivery adds further pressure, so haemorrhoids can appear or worsen in the days after childbirth. The good news is that pregnancy-related haemorrhoids often improve in the weeks following birth, and the same gentle self-care measures apply. If you are pregnant or recently gave birth, check with your doctor or midwife before using any medicated cream.
Diet, Lifestyle & Genetics
- Low-fibre diet and constipation: hard stools and straining are a leading trigger. Fibre softens stool and reduces the need to strain.
- Prolonged sitting or a sedentary routine increases pressure on the anal area.
- Being overweight adds pressure on the pelvic veins.
- Heavy lifting and repeated straining can bring on or worsen symptoms.
- Frequent diarrhoea can irritate the area.
- Ageing, as the supporting tissues naturally weaken over time.
- Family history: a tendency to haemorrhoids can run in families.
Treatment & Relief
Most haemorrhoids improve with self-care. If symptoms persist, several effective clinic and surgical options are available, and the right choice depends on the type and grade.
Home & Lifestyle Measures
- Eat more fibre — wholegrains, fruit, vegetables and legumes — and consider a fibre supplement if needed. Increasing dietary fibre is one of the best-supported ways to ease symptoms and reduce bleeding.
- Drink enough fluid so the added fibre can soften stool rather than worsen constipation.
- Avoid straining and try not to sit on the toilet for long periods.
- Warm sitz baths — sitting in a few inches of warm water for 10–15 minutes once or twice a day — can soothe soreness.
- Over-the-counter creams, ointments or suppositories may relieve itching and discomfort for short periods. A pharmacist can advise; if you are pregnant, check first.
- Keep the area clean and pat dry gently rather than rubbing.
Medical & Surgical Options
If self-care does not settle symptoms, a colorectal doctor can examine you and discuss clinic-based or surgical treatments. These may include:
- Rubber band ligation — a small band is placed around the base of an internal haemorrhoid to cut off its blood supply so it shrinks and drops off. It is a common clinic procedure for internal haemorrhoids.
- Sclerotherapy — a solution is injected to shrink the haemorrhoid.
- Infrared coagulation — heat is used to shrink smaller internal haemorrhoids.
- Haemorrhoidectomy — surgical removal, generally reserved for large or persistent haemorrhoids, or those that have not responded to other measures.
If your symptoms are persistent, recurring or affecting daily life, a colorectal specialist can examine you and explain which treatment suits your situation.
Diagnosis & When to See a Doctor
A doctor can usually diagnose haemorrhoids from your history and a simple examination. This may include a visual check, a digital rectal examination (a gloved, lubricated finger) and, for internal haemorrhoids, a short look inside with an anoscope. These steps also help rule out other causes of the same symptoms.
You should arrange to see a doctor if you notice any of the following:
- Bleeding that persists, recurs, or is heavy.
- Symptoms that do not improve after about a week of self-care.
- A painful or hard lump at the anus.
- A change in your usual bowel habit, or stools that look darker than usual.
- You are aged 45 or older, or have a family history of bowel cancer.
Rectal bleeding is common with haemorrhoids and is usually not serious, but it can occasionally be a sign of another condition. It is sensible to have new or persistent bleeding assessed rather than assuming the cause.
Prevention
The same habits that ease haemorrhoids also help prevent them:
- Keep fibre and fluid intake up to maintain soft, regular stools.
- Go when you need to, and avoid straining or sitting on the toilet for long stretches.
- Stay active and avoid long uninterrupted periods of sitting.
- Maintain a healthy weight.
- During pregnancy, manage constipation early with your doctor or midwife’s guidance.
Frequently Asked Questions
What do haemorrhoids look like in women?
Internal haemorrhoids sit inside the rectum and usually cannot be seen from the outside. External ones look like soft swellings or lumps around the anal opening, and a thrombosed haemorrhoid looks like a firm, bluish-purple lump. They look the same in women as in men.
What are the symptoms of haemorrhoids in females?
Itching or irritation, discomfort or pain (especially when sitting or passing stool), a lump near the anus, and bright red bleeding. Symptoms can flare during and after pregnancy.
How do you get rid of haemorrhoids?
Many cases settle with more fibre and fluids, not straining, and warm sitz baths. Over-the-counter creams may help symptoms. If these do not work, a doctor may suggest a clinic procedure such as rubber band ligation or, for larger haemorrhoids, surgery.
Can pregnancy cause haemorrhoids?
Yes. Increased pelvic pressure, hormonal changes, constipation and straining during delivery all make haemorrhoids more likely during pregnancy and after birth. They often improve in the weeks following childbirth.
Can you get vaginal haemorrhoids?
Haemorrhoids form in and around the anus, not the vagina. A swelling felt near the vaginal area is more likely a vaginal or vulval varicose vein, which a doctor can distinguish on examination.
Are haemorrhoids different in women than in men?
The condition is the same. Women simply have extra triggers — mainly pregnancy and childbirth — and may notice discomfort during intercourse if an external haemorrhoid is present.
When should I see a doctor for haemorrhoids?
If bleeding persists or recurs, symptoms do not improve after about a week of self-care, there is a painful lump, or you have a change in bowel habit. Rectal bleeding should always be assessed, especially from age 45 or with a family history of bowel cancer.
Do haemorrhoids go away on their own?
Mild haemorrhoids often settle within days to a couple of weeks with self-care. Larger or recurring ones tend to return and may need a clinic procedure or surgery.
Conclusion
Female haemorrhoids are common and, in most cases, manageable. Knowing the type, recognising the symptoms and starting simple self-care early will resolve many cases. When symptoms persist, recur or include rectal bleeding, an assessment by a colorectal specialist gives you a clear diagnosis and a treatment plan suited to you.
References
- Johns Hopkins Medicine. Hemorrhoids. hopkinsmedicine.org
- Cleveland Clinic. Hemorrhoids: Symptoms, Causes & Treatment. my.clevelandclinic.org
- Harvard Health Publishing. Hemorrhoids and what to do about them. health.harvard.edu
- National Institute for Health and Care Excellence (NICE) CKS. Haemorrhoids. cks.nice.org.uk
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), NIH. Hemorrhoids. niddk.nih.gov


